[-]
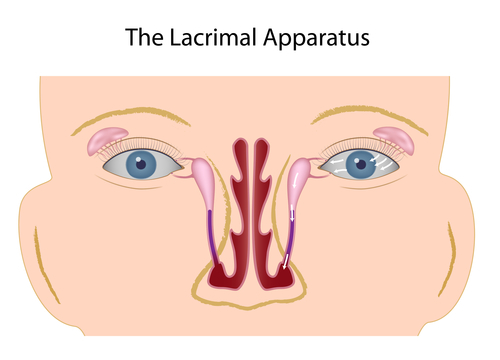
Tearing of the eye is, usually, a consequence of delayed tear elimination from the ocular surface, due to a narrowing or complete blockage of the tear drainage pathways. Most frequently, the problem is in the main tear duct, which transports tears from the tear sac to the nose. Less frequently, the small canals (canaliculi), which convey the tears from the eye to the tear sac, are affected.
In the case of a watery eye, the eye and eyelids are examined under the slit lamp (microscope). The tears are stained with a special dye (fluorescein), in order to assess their delayed elimination/retention and where they overflow on to the eyelid and cheek skin. This type of assessment and applying pressure on the tear sac, are all that can be done in children, and the rest of the exam is carried out in general anesthesia, directly prior to the surgical intervention.
Next, a special rigid endoscope is used to view the inside of the nose (nasal endoscopy). If the tear pathways are patent, orange due can be seen flowing into the nose.
After this, a special blunt cannula is used to, painlessly, inject fluid through the tear ducts (syringing). In simple terms, this exam helps us to differentiate narrowing from complete obstruction of the ducts.
In most cases, these procedures are enough to make a diagnosis and to indicate which type of procedure is needed. In a small number of specific cases, additional specialized investigations are needed.
As is the case with other types of surgery, the preparation depends, mostly, on the planned type of anesthesia. In small children, all procedures are done in general anesthesia.
In adults, surgical procedures can be done in local or general anesthesia.
Local anesthesia is usually combined with intravenous analgo-sedation (intravenous administration of painkillers and sedatives).
Depending on the type of anesthesia and complexity of surgical procedure, different labwork and specialist consults need to be prepared in advance.
It is very important that all medicines and supplements, which affect the blood clotting mechanism, are discontinued in time.
If this matter is not addressed properly, there is an elevated risk of bleeding, due to the rich blood supply of the nose and surrounding region.
Operation of the main tear duct (DCR) can be performed via a skin incision (external DCR), or through the nose (endonasal DCR). The advantage of the latter method is the absence of a skin incision (and visible scar), as well as a faster post-operative recovery. Doctor Zoran Zikic is currently the only eye surgeon in the region of the former Yugoslavia, who, independently, performs this procedure (you tube). This procedure needs to be done under general anesthesia.
Externall DCR is performed if the health status of the patient requires that the procedure be done in local anesthesia, as well as in complex cases (narrow nose, previous bone fracture etc.)
In both procedures, a silicone stent is placed inside the newly formed passage, and is removed, in the office, one month after the operation.
In babies, with a blocked tear duct, the procedure consists of nasal endoscopy, probing, syringing and insertion of a special silicone stent, in general anesthesia. The special silicone stent (Mono K) is removed in the office, after three months.
If the small tear ducts (canaliculi) are blocked, a special glass tube needs to be implanted (conjunctival-DCR with a Lester Jones tube).