The tearing or watery eye is a relatively common problem, either in infants or in adults. The eye may be wet only on one, or on both sides, constant or intermittent. For example, during a common cold, the mucous membranes in the nose are swollen, which causes the tear duct to be temporarily blocked. In this case, when the cold resolves, so does the increased tearing.
On the other hand, increased wetting of the eye may be a sign of certain diseases of the eye, or of the nose or sinuses. The problem may be congenital or acquired.
In the case of congenital blockage of the tear duct, symptoms are present at birth or in the first few months, in the form of increased tearing and secretion. This causes increased anxiety in parents, who frequently resort to overuse of antibiotic eye drops and ointments. Bearing in mind the fact that the cause of this problem is mechanical, it is clear that topical antibiotic use cannot solve this problem, however long term use can lead to bacterial resistance. This is why parent education is important, on the first visit to an eye specialist, regarding the natural evolution of this problem, as well as the therapeutic possibilities.

Tearing in a newborn child
In more than 90% of cases, this problem resolves by itself during the first 12 months of life, by spontaneous rupture of the membrane, which is blocking the duct. For this reason, in this period, only conservative neasures are advised, such ase tear sac massage (to express the accumulated secretions) and lid hygiene. If spontaneous resolution does not occur until the child is one year old, it is neccessry to perform an intrevention in general anesthesia, during which the nose is examined with an endoscope, the tear duct is probed with a special instrument to locate and penetrate the blockage, and a special silicone stent is inserted. The stent is removed after 3 months, in the office, without the need for any other anesthesia but eyedrops.
There are more complex causes of congenital blockage of the main tear duct, and/or small tear canals, which conduct tears from the eye to the tear sac and to the begining of the main tear duct. In these cases the surgical procedures are also more complex and involve the creation of a new tear duct and sometimes the insertion of a special glass tube.
In the case of an acquired watery eye, during the initial eye exam, one needs to rule out reflex tearing, which can be caused by eye irritation. The leading cause of reflex teraing are dry eye syndrome and blepharitis (inflammation of the eyelid margin), as well as allergic conjunctivitis (inflammation of the mucous membrane of the eye).
Tears can overflow even if the tear drainage system is patent, as a consequence of poor eyelid tone (laxity), or defective position (inverted, everted), as well as inthe case of eyelid muscle paralysis (facial nerve damage).
Bearing in mind that the tear duct ends in the nose (nasal) cavity, we can understand why disorders of the nasal and sinus mucosa can affect its function. Chronic inflammation of these structures (rhino-sinusitis) is a frequent finding in patients with a narrowed or blocked tear duct(s).
Acquired problems with the tear outflow apparatus can also be caused by certain medications and radiotherapy. Injuries to the inner part of the eyelid can damage the fine small tear canals (canaliculi), whereas fractures of the facial bones can involve the bony tear duct.
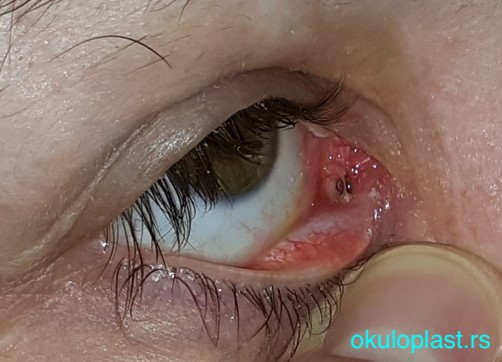
However, in the majority of cases, there is a progressive narrowing of the tear duct, due to a swelling and thickening of its mucosa, the exact cause of which is still not clear. It is more frequent in women and can increase with age. In the begining the tearing is intermittent, usually in cold and windy conditions. With time, the waternig becomes constant, the first sign of infection being stickyness of the eye due to increased presence of mucus in the tears. With progression the mucus turns to puss, which can be expressed by pressure on the tear sac. This, so called, chronic infection of the tear sac, can worsen by becoming acute, when the tear sac is hard and painfull. This condition needs to be treated with systemic antibiotics.
 chronic inflammation of the tear sac
chronic inflammation of the tear sac acute inflammation of the tear sac
acute inflammation of the tear sacThe definitive solution is only by a surgical intervention, the aim of which is to create a new passage for tears, from the tear sac to the nasal cavity. Whichever technique is used to achieve this, it si important that the created communication remains opern with time. The operation can be carried out through a skin incision or through the nose (with an endoscope), or by a laser, in general or local anesthesia, depending on the health status or preferrence of the patient. In any case, after the surgery, it is important to do regular endoscopic follow ups, so that crusts in the nose can be cleaned, in order to avoid closure of the newly created opening.
A separate issue is the acquired narrowing/blockage of the small tear canals (canaliculi). This can be a consequence of viral infections, autoimmune diseases of the eye mucosa, as well the use of certain types of topical or systemic medications. Since, in these cases, the tears do not reach the tear sac, the tears are clear and there is no stickiness.
The surgical procedures are more complex. If it is possible, a resection of the damaged part of the canaliculus is performed, after which the healthy parts are anastomosed (reconnected), and a silicone stent inserted. The stent is removed after 6 months. If this is not possible, or does not yield a satisfactory result, the alternative is the insertion of a special glass tube, which conveys the tears, directly from the eye to the nose.
 Glass (Lester Jones) tube, viewed from the outside
Glass (Lester Jones) tube, viewed from the outside Glass (Lester Jones) tube, viewed from the nose
Glass (Lester Jones) tube, viewed from the nose